Foreword
In my December 2025 Reflections and Initial Impressions report, I set out what I had heard from my initial engagement with women and families, community organisations and staff. I have undertaken significant further engagement since then.[1] To date, my team and I have met with over 400 family members, and we have heard from over 8,000 people through the public call for evidence so far. I would like to thank everyone for taking the time to engage with us – I know that this has come at considerable emotional cost.
I have not yet finished evidence gathering and analysis, but I wanted to share the insights I have gained so far, which reflect what families, staff and others have told us and what the investigation team has seen. As we are midway through the investigation further themes and issues may yet emerge, so no firm conclusions or recommendations are made in this interim report.
The experiences described by women and people who have been pregnant, families and non-birthing partners in my December report have remained as consistent themes during our meetings across the country. We have heard about families being disregarded and not listened to during pregnancy and labour, a lack of kindness and compassion, and reluctance on the part of trusts and professionals to admit mistakes and say sorry when things have gone wrong.
In the absence of clear explanations, women often wrongly blame themselves if their babies are harmed or die – they think it is because of something they have done or that they should have been more insistent that there was a problem. Women and families have told us about the high levels of distress, pain and suffering that are caused when death or serious harm occur, leading to psychological trauma and a loss of trust, which is compounded when the system fails to respond quickly and appropriately. We have been told about a lack of consistency in the provision of care, which has been described as a ‘postcode lottery’ by women, families and staff – from my perspective as someone outside the health and care system, this looks like a fragmented service. We have seen instances of care being delivered in wholly inadequate estate facilities. The system is not working for women, babies and families, or for staff.
Time and time again, families who have engaged with the investigation say that they are doing so because they do not want the same to happen to any other family. And yet they are seeing the same failures repeated. It is also a source of continuing distress to families, and great frustration to staff, that the areas identified in previous reviews and investigations as requiring action do not seem to have been addressed or have only been partially addressed. This cycle must stop.
“I will be at peace when changes are made and I’ve been able to contribute to this. That is the driving force for me.” [Family member]
Ten years ago this month, a vision for safe, kind, family-friendly maternity services for all women and families in England was set out in a report titled ‘Better Births’.[2] During the decade that has passed since then, maternity services have experienced significant challenges, including the extreme pressures created by the COVID-19 pandemic. Overall, rather than delivering the Better Births vision, the maternity system is struggling to meet the demands of increased pressures and greater clinical complexity. We have seen maternity and neonatal services trying to respond in difficult circumstances and dealing with competing pressures, but too often failing to deliver the safe care that women, families and babies expect and deserve, at times with devastating consequences.
Safe and equitable maternity and neonatal care should follow a journey or ‘continuum of care’. What do I mean by that? That: women need care prior to pregnancy; while they are pregnant (antenatal care); during labour and birth; immediately after birth, and in the six weeks after that (postnatal care). This continuum also includes, where necessary, specialist neonatal services for babies, and support for families following bereavement or harm. The maternity pathway should connect seamlessly with other services including public health, mental health, GPs and social care – when it works well, this pathway can positively influence the future life course of a mother, baby and their wider family. [3] Pregnancy and birth are major life events for everyone involved. We must get it right.
This investigation is not operating in a vacuum. There is a wider societal context which includes persistent and pervasive socio-economic and gender inequalities, as well as societal norms and attitudes that influence how women are perceived. In addition to the emotional harm that families experience when something goes wrong, there are long term economic, psychological and emotional consequences and costs for families and society. These include relationship breakdown, mental health and depression, impact on ability to work, and reduced life chances for children who may need life-long support for their disabilities from social care, housing, education and welfare services.
The increased use of social media, which has enabled greater access to online support and information, has changed how women and families interact with the NHS. In many instances this has been a positive development with women able to share experiences and educate themselves, helping them to better navigate their way through pregnancy and childbirth. However, misinformation and lack of nuance can distort perceptions and understanding of risk.
I have been asked many times during the course of this investigation what makes it different to those investigations and reviews that have gone before. The answer is that this investigation is national in scope and takes a whole system view – looking at people, culture, organisation, processes, infrastructure and the wider factors impacting on the care delivered by maternity and neonatal services. I see it as my purpose to understand the context and identify the urgent systemic issues that must be addressed. This includes: understanding why negligent, poor, good and excellent practice can coexist; the drivers of consistent, sustained and safe care; and how these drivers can be replicated.
There remain persistent inequalities within the maternity and neonatal system, with notably higher risks of adverse outcomes for women from Black and Asian backgrounds and women living in more deprived areas.[4] Of great concern to me are the levels of racism and discrimination we have heard about, exhibited by staff towards women and families, between staff, and by women and families towards staff. Racism can be structural and, whilst these attitudes may stem from wider societal stereotypes, there is no place for racism and discrimination in an NHS which – in the opening words of the NHS Constitution – ‘belongs to the people’. Class, race, income and other differences should not matter in an NHS which provides a comprehensive service and ‘aspires to the highest standards of excellence and professionalism’ and where ‘the patient is at the heart of everything the NHS does’. These are the basic principles and values which guide the work of the NHS.[5]
My thanks to the NHS staff who have engaged with the investigation so far. I have heard from many committed staff who want to improve services and provide safe care, but they have also highlighted cultures of blame and fear, and a failure to deal with poor professional conduct. Strong, principled leadership is critical to addressing these cultural issues, which hinder professionals’ capacity to consistently deliver compassionate and safe care.
In this report I set out the background and changing context in which maternity and neonatal care is provided. I go on to examine six factors that could be contributing to the pressures on the maternity and neonatal system. These are as follows:
- Capacity pressures
- Culture and leadership
- Racism and discrimination
- Poor responses and lack of accountability when things go wrong
- The quality of estates
- Workforce
The report concludes with next steps. I remain committed to driving the change which is so clearly needed in the maternity and neonatal system.
Baroness Valerie Amos
Chair, Independent National Maternity and Neonatal Investigation
26 February 2026
Part 1: The changing context of maternity and neonatal care
- The maternity and neonatal system is operating in a markedly different environment today compared with even a decade ago. In looking to understand the changing context, there are three major factors which I would like to point to – changes in outcomes for women and babies over time, changing demographics, and increasing clinical complexity.
- Firstly, there have been changes in outcomes for women and babies over time. In 2016, the then government set a national ambition to halve (from 2010 levels) the rates of stillbirths, neonatal mortality, maternal mortality and brain injuries by 2030. In 2017, the government brought the deadline forward to 2025 and added a separate ambition to reduce preterm birth rates from 8% to 6%.
- Despite initial decreases after 2016, progress reversed or stalled during and following the COVID-19 pandemic. Stillbirth, neonatal mortality, and preterm birth rates have started to decrease again in recent years.[6] Concerningly, the maternal mortality rate increased from 8.8 (per 100,000 maternities) to 12.8 (per 100,000 maternities) in the period between 2017 to 2019 and 2022 to 2024.[7]
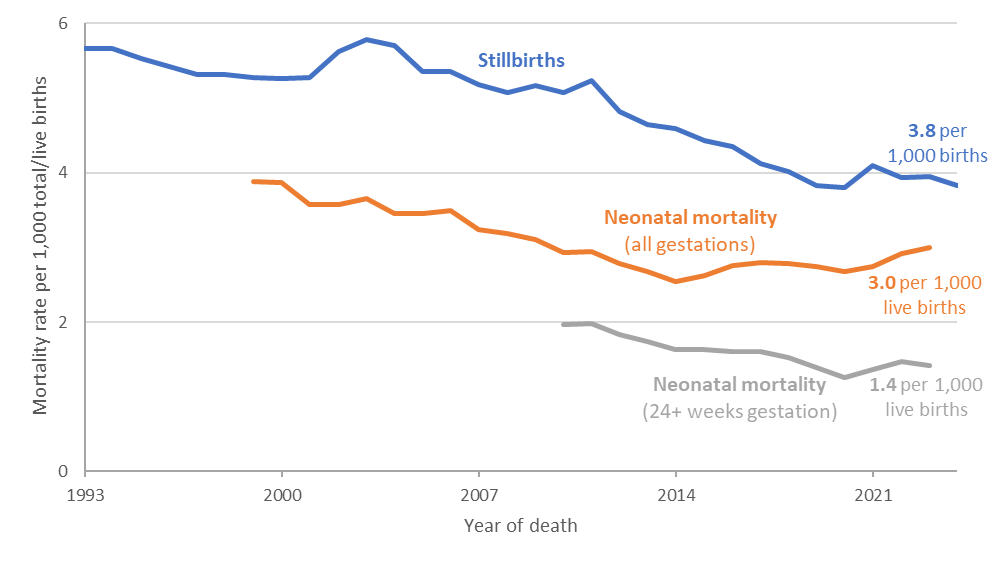
Figure 1: Stillbirth and neonatal mortality rates in England, 1993-2024[8]
- Secondly, the demographic, social and health profile of women using maternity services has changed over time, reflecting wider societal shifts and national trends in public health.
- Women are now giving birth at older ages: in 2024, 61% of live births were to women aged 30 or older, and 26% were to women aged 35 or older. In contrast, in 2004, 49% of live births were to women aged 30 or older, and 19% were to women aged 35 or older.[9] There has also been an increase in the number of pregnant women with pre-existing health conditions.[10] These factors are associated with a higher likelihood of developing complications during pregnancy, in labour and after birth, and highlight the need for a maternity and neonatal system that is equipped to meet the needs of a changing population.
- We also know that some groups of women face higher risks than others. National data from MBRRACE-UK demonstrates consistently higher maternal mortality rates for Black and Asian women: Black women are almost 3 times as likely to die during pregnancy or up to 6 weeks after birth compared with White women, and Asian women were 1.3 times more likely to die during the same period.[11] Women living in the most deprived areas have twice the rate of maternal mortality compared with those in the least deprived areas.[12] These differences reflect long‑standing inequalities, including the effects of disadvantage, racism and discrimination.
- These wider societal factors point to the importance of a national, proactive response to ensure that services can meet the needs of the women and babies they care for, including the provision of additional care and services for women who enter pregnancy with social disadvantage.
- Thirdly, alongside demographic changes, the nature of interventions has changed. In 2024 to 2025, labour began spontaneously in 42% of births, a decrease from 59% in 2014 to 2015. Rates of induction rose throughout the 2010s although decreased between 2020 to 2021 and 2024 to 2025, and rates of instrumental birth decreased slightly from 13% in 2011 to 2012 to 11% in 2024 to 2025. Rates of caesarean birth have increased, from 25% of births in 2011 to 2012 to 45% of births in 2024 to 2025, with a significant proportion of this increase within the past 5 years.[13]
- Rates of planned caesarean births (a caesarean section scheduled in advance of labour) doubled between 2011 to 2012 and 2024 to 2025, from 14% to 28% of births, and rates of emergency caesareans (an unscheduled caesarean section performed because of complications arising during pregnancy or labour) increased from 11% to 17%.[14] In the same period, rates of caesarean births in other OECD countries and the USA have remained relatively stable.[15] For example, between 2014 and 2024 rates of caesarean section in the USA increased from 32.2% to 32.4% despite the USA also seeing increases in maternal age and pre-existing health conditions.[16]
- The drivers behind increased interventions are complex, and it is not our intention to infer that such interventions constitute inappropriate care. Indeed, previous reviews have found that a culture of avoiding intervention in some trusts, even when clinically necessary, resulted in avoidable harm.[17] [18] It is, however, important to take these changing levels of intervention into account when considering how maternity and neonatal services should be designed and delivered.
- In addition to the changing context set out above, it is important to take into account the fact that maternity and neonatal services operate within a complex set of oversight and accountability arrangements within geographical boundaries which do not always align. Maternity services are delivered locally but have complex commissioning and governance structures including Local Maternity and Neonatal Systems (LMNS), Integrated Care Boards (ICBs) and NHS England National and Regional oversight. Neonatal services sit under Operational Delivery Networks (ODNs), which coordinate neonatal services to ensure babies receive care in the most appropriate setting, bringing together neonatal units (Neonatal Intensive Care Units, Local Neonatal Units and Special Care Units), transport services and specialist teams to manage neonatal cot capacity, neonatal pathways and neonatal clinical standards. These structures have been subject to change over the past few years.
Part 2: Factors which are creating pressure on maternity and neonatal services
- We have identified six factors which could be contributing to the pressures on the maternity and neonatal system:
- Capacity pressures
- Culture and leadership
- Racism and discrimination
- Poor responses and a lack of accountability when things go wrong
- The quality of estates
- Workforce
We examine each of these in greater detail below.
Capacity pressures
- We have heard about capacity pressures at every stage of the maternity journey. We have also identified inconsistencies between individual units and in the birth choices available to women, sometimes as a result of these capacity pressures. Some variation is appropriate as NHS trusts consider the needs of their local communities when putting services in place, however too often we heard about services that had been depleted or even stopped because of capacity pressures. Examples include:
- Women, midwives and obstetricians said that antenatal appointments were often not long enough to discuss a woman’s pregnancy meaningfully – particularly for women with complex health needs. Some also reported inconsistent provision of antenatal classes, which could contribute to the need for longer appointment times;
- Women and families reported waiting many hours for medical assessment, review or clinical opinion in Maternity Day Assessment Units and triage areas (assessment areas that provide care between planned appointments in maternity);
- We heard that some antenatal wards and delivery units are stretched, resulting in delays to admissions, progression for induction, and planned caesarean sections;
- Community midwives told us how they were moved to work in delivery units in hospitals to cover staffing gaps, compromising care in neighbourhood settings and disrupting continuity of care. This also impacts on safety, as staff predominately working in one area said they were not always familiar with working practices in another;
“We’re called into a busy delivery suite and we’re called in because it’s gone bonkers and it’s not our familiar area. So we are half the time having to ask people what to do. We’re not providing the same service that the delivery suite midwives can do because they know it like the back of their hands.” [Midwife]
- In some areas home births had been suspended for safety reasons as a result of a lack of staffing;
- Staff from postnatal wards were frequently redeployed to delivery units to maintain staffing levels, creating capacity pressures. These pressures were compounded by the increasing complexity of the needs of mothers and babies, and higher numbers of caesarean sections which require longer postnatal stays;[19]
- The provision of transitional care on maternity units differed across trusts with variation in whether a mother and baby needing transitional care can remain together on the postnatal wards;
- Neonatal community outreach teams had varied approaches across trusts in how soon a baby can be discharged home from a special care baby unit and transitional care ward;
- There were differences across trusts in the care choices and place options for babies who needed neonatal palliative care.
- Delays in providing early senior clinical review, particularly in relation to decisions about care and treatment, were frequently reported across the maternity journey. When there is pressure on assessment areas, delivery units and postnatal wards, it is unsurprising that women and families report a lack of basic care and support.
- Day assessment and triage areas have become focal points for acute and sometimes emergency antenatal care, often without the staffing levels, senior decision-making capacity or estate provision required to deliver safe, high-quality care on a 24-hour basis. We noted that some services had taken steps to address these capacity pressures and improve the ‘flow’ for women and families through their journey in hospital. However, many women who had recently given birth spoke of the difficulty getting through to triage units on the phone, experiencing long waiting times, or reported that they had been sent home without being given a thorough assessment. Some units we visited had recently redesigned their triage services, including increasing the number of senior obstetricians and staff to answer families’ phone calls and prioritise assessments.
- The layout and geography of maternity and neonatal units can support or hinder continuity of care and ‘flow’ between different stages of the maternity and neonatal journey as well as between different clinical locations. For example, we heard that when areas such as triage, theatres, postnatal wards and the neonatal unit are physically close together, this reduces the time that women and families have to wait for a medical review or for a free bed, as well as enabling close teamworking for staff. Additionally, co-location of services facilitates safe, personalised care. For example, families told us that it allows them to move more easily between areas without having to rely on support staff, including being able to visit their babies in a neonatal unit.
- Inefficient IT systems create additional pressures for staff and create stress for women and families. Patient information and notes are stored on multiple systems and, in some cases duplicated on paper records, requiring manual transfer of information which consumes time and creates a patient safety risk as it can result in missing information. IT systems are often not intuitive and are not interoperable with each other or with wider hospital IT systems, such as those used for pathology and radiology. Staff spoke about the risks involved in having to provide care and document it simultaneously, and of having to access multiple IT systems at once, particularly during an emergency.
- We heard from multiple women and families about the impact of missing or incomplete records – including concern that clinical decisions are being made without access to all the requisite information. We also heard from families that staff did not appear to have read notes before their appointments, meaning that they had to repeat their medical needs and previous care history frequently. This can cause distress for families who have had previous traumatic experiences and left some families feeling that staff did not care.
Culture and leadership
- Organisational culture is vital in determining the safety and effectiveness of maternity and neonatal care. Culture has been described as the shared ways of thinking, feeling, and behaving in (healthcare) organisations.[20] [21] and a growing body of evidence links culture with quality outcomes.[22] Culture is also vital in shaping women’s and families’ experiences of pregnancy, childbirth and postnatal care through the delivery of an equitable service. However, we heard from many families of striking shortcomings in these areas, and we heard from staff of the challenges they face in sustaining and improving a compassionate culture.
- Teamwork is vital in high stress situations. In some trusts, we heard troubling accounts from staff of poor relationships between team members. It is important for obstetricians and midwives to work effectively in teams, respecting each other’s expertise and having a shared approach to common objectives. The same is true for team working between maternity and neonatal teams. There is a great deal of evidence that this does not always happen – the effect on care of differing approaches can be disastrous.
- Culture is inextricably linked with leadership. To be effective, clinical leaders need training, time and support, but we heard that this was often not the case. Clinical teams are influenced by the attitudes and behaviour of those in senior positions, and if these are poor the effect on culture and teamworking is detrimental. Effective clinical leaders are crucial to ensuring the safety and effectiveness of services, and in initiating action when standards are not being met. They provide an important link to the Board.
- We have heard that there are differences in the way that clinical directors (doctors responsible for medical leadership of a unit such as a maternity unit) work compared with directors and heads of midwifery. For example, clinical directors can be appointed on a temporary basis, to be succeeded by another consultant in turn after a few years; whereas directors and heads of midwifery tend to be longer-term appointments. We heard clear support for the role of director of midwifery and the importance of close working with the Board, visibility in clinical areas and being accessible to staff.
[Note: This paragraph was amended on 3rd March 2026 to include references to Directors of Midwifery.] - We saw examples of effective leadership which had led to families and staff reporting more positive experiences. For example, with strong support from those at executive level, some trusts have introduced family integrated care (FiCare) models which actively involve families in decision-making and in supporting their baby’s care. We also heard that strong relationships between maternity and neonatal leadership enable an integrated approach to care.
- We heard from staff about clinical leaders and trust management not always dealing with poor behaviour from some senior clinicians. Staff described instances where conduct fell markedly short of social and workplace norms, including verbal aggression, refusal to carry out designated functions such as attending handover rounds or callouts at night, and sometimes bullying and racist behaviour. In these instances, some staff felt definitive action was rarely taken, and instead they were expected to work around the problem, often leading to frustration and poor morale.
- Staff told us about the amount of public scrutiny and criticism that they have experienced, and the impact this can have on their mental health. We heard from midwives who hide their name badges or uniforms in public or lie about their jobs when meeting people outside of work. We also heard about staff experiencing burnout.
“Please, can you tell them we need help to put pride back into our profession?” [Midwife]
“I feel embarrassed to say I am a midwife now.” [Midwife]
“That’s why people get sick, don’t they because they’re absolutely burned out and they’ve also got families at home that are also struggling with the choice of career you’ve picked to make your family life better.” [Midwife]
Racism and discrimination
- When looking at culture, it is essential to consider the extent to which racism and discrimination are present, tolerated or actively addressed within organisations, and how systems respond when racist and discriminatory behaviours, policies and practices are uncovered.
- Systemic and interpersonal racism within maternity and neonatal care is widely recognised and cited as a factor contributing to racial inequities reported in maternity and neonatal outcomes.[23] [24] [25] [26] Throughout our investigation, we have heard about unacceptable racism and discrimination across the maternity and neonatal system.
- Inequalities extend to babies’ outcomes. Babies of Black ethnicity are more than twice as likely to be stillborn,[27] and are at increased risk of preterm birth[28] and neonatal admission at term[29] when compared with White babies. Neonatal mortality rates are also higher for Black and Asian babies compared with White babies,[30] and there is variation in neonatal care delivery between ethnic groups.[31] Stark inequalities are also evident by socioeconomic status. Maternal and neonatal mortality rates are twice as high for women living in the most deprived areas of England compared with women living in the least deprived.[32]
- There is more limited information available on outcomes for women and families with disabilities, refugee and asylum women, LGBTQ+ people, and people from Gypsy, Roma and Traveller backgrounds. This means that some forms of discrimination remain under-recognised. The Investigation is engaging with a wide range of families and stakeholders to understand the experiences of minority and marginalised communities.
- We have heard about stereotypes being used in maternity and neonatal services and the impact this has on families’ trust in and engagement with services. This includes accounts of Asian women being stereotyped as “princesses”, with the implication that they are overly demanding or unable to cope with pain. During a stakeholder panel on one of our local trust visits, a community organisation reported a hospital staff member who trained students saying, “the bloody Asian ones just go on and on and on”.
- Black women reported being deemed as having ‘tough skin’ and able to tolerate pain. During a family evidence panel one woman said, ‘I feel like, for us black ladies, they feel like we can handle the pain, even when we are complaining we are in pain”. Black women described experiences of ‘the angry or aggressive Black woman’ stereotype impacting their care. One woman said, “I was begging for help… I was made to feel like I was that aggressive, angry Black woman. But that isn’t me.”
- Black women also described feeling that they had to advocate for themselves more forcefully due to their ethnicity. One family told us “a midwife came back into my room and said, ‘you’re Black, you’re mixed race, you need to speak up if anything happens’”. Despite the need to speak up for themselves, some families described feeling compelled to “moderate”their behaviour to avoid racial stereotyping in maternity care.
- Community organisations we have spoken to have described how racism, discrimination and culturally inappropriate care can result in ethnic minority families feeling that the system is “not for them”, resulting in eroded confidence and trust in maternity services.[33] [34]
- We heard about families experiencing a lack of sensitive and culturally competent communication, particularly when clinicians discussed risks in pregnancy or recommended additional care. Some Black women told us that explanations for clinical decisions were poorly delivered and sometimes reduced to “it’s because you are Black,” leaving them feeling stigmatised.[35] Several women described declining or being hesitant about accepting medical advice when communication felt insensitive or discriminatory.
- We have also heard about staff experiencing racism and discrimination in a myriad of ways. Some staff members have told us how they have been turned away from giving care to patients because of their ethnicity or background; whilst others have told us about systemic racism within the trust itself.
“I feel the culture, maybe I was naïve as a junior consultant, I didn’t have any fear, and I felt that the people that I spoke to listened. And then as I matured in the profession, maybe I became more brave to knock on more doors. I’ve been, felt racially abused basically; I’ve made complaints formally. The trust hasn’t acknowledged that. There’s been an external review which has identified racism and discrimination and bullying and harassment. There’s been no action to address that.” [Consultant]
- Families and organisations have also described their experiences of discrimination. Many told us that current systems and attitudes still fall short of what is expected. Much of what we heard is supported by published evidence. [36] [37] [38] [39] A few of the many examples we heard are set out below:
- Muslim families described feeling discriminated against on the basis of their religion and feeling unable to raise concerns due to fear that discriminatory attitudes may result in poor treatment for their baby. For example, a parent listening to Qur’anic recitation was told by a nurse to “turn it down; I don’t want to hear it”.
- Families with pre‑existing physical or mental health conditions described inaccessible buildings, insufficient adjustments and feeling stigmatised or dismissed based on their health condition, for example, guide dogs being refused entry and essential equipment such as hoists or accessible facilities not being available.[40] One parent with a pre-existing physical health condition noted, “I have had very senior midwives say, “we don’t see many of you””.
- One woman reported being told she was “too fat to have children”, when seeking support after multiple pregnancy losses. Another woman recalled being called by a consultant who “ran through the list of things that were going to happen to me because of my BMI: I was going to get gestational diabetes, I was going to get preeclampsia, my baby was going to get stuck on the way out because of shoulder dystocia, and that would probably lead to brain damage”.
- Families who speak English as an additional language, or who require British Sign Language interpretation reported that insufficient availability of professional interpreters led to confusion, distress and fear. One family recounted: “They didn’t use a translator… and all he heard was ‘baby dead, wife really poorly”. Although healthcare professionals described improvements in interpretation services, they emphasised that these improvements are from a low baseline. Persistent challenges include limited availability of interpreters for specific languages or dialects, unreliable remote interpreting technology, and interpreters of inappropriate gender for sensitive discussions.
- LGBTQ+ families reported a lack of inclusivity, with some reporting that services focus narrowly on “mothers” and “fathers” and fail to reflect diverse family structures. One family member said “I almost died in birth, as I had my baby – I was then asked questions like ‘who was the real mum?”
- Young parents described facing judgement and discriminatory attitudes and felt that their grief and trauma were minimised because of their age. One parent who had lost twins at 17 shared: “He’d completely written me off… didn’t care that I’d lost twins.” Another recalled being told, “You’re young, you’ll be fine, just try again,” despite having experienced multiple losses.
- Families told us that they value services which focus on reducing practical barriers and building trust, including outreach delivered in partnership with voluntary and community organisations. This is supported by stakeholders we have spoken to, who highlighted the important role that trusted community organisations and faith leaders could play in facilitating earlier engagement with services. These community groups often have longstanding relationships with communities and are well placed to share information, support navigation of services, and build confidence and trust in the safety and relevance of maternity care. They are vital – however they are funded outside of the national system, resulting in a “postcode lottery” and uncertainty about future funding. Other supportive interventions include flexible appointment systems, community-based or home-based antenatal services and bilingual health advocates.
Poor responses and a lack of accountability when things go wrong
- Families described a lack of compassion in the aftermath of incidents that had resulted in harm, including birth trauma and baby loss. We have repeatedly heard from women and families about a lack of transparency, clear communication and learning when things went wrong. For example, families have reported not being offered the chance to be involved in investigations from the outset, not being advised when investigations had concluded, or not being sent copies of reports.
“They did the PMRT [Perinatal Mortality Review Tool] obviously, following his death. I really struggled with that because for me, I wanted to have a part of — I wanted to be part of that investigation. They said we weren’t allowed to go to any of the meetings. I sent over email views that I wanted to be recorded to reflect what we felt around the care. They were never included.” [Family member]
- Families also reported that access to investigations can feel arbitrary and unfair, and that even when there is an investigation these can be of poor quality and do not accurately reflect the events which took place.
- We were told by families that in some instances staff found it difficult to talk to them after a bereavement and that they experienced reluctance from staff to admit that care had not met the expected standards, despite their legal duty of candour. We heard from many families about feeling that there had been a ‘cover up’ and defensiveness from NHS trusts, the resistance they faced from trusts when requesting their notes, and instances of medical notes being amended or redacted.
“So I’d initially requested my medical notes on paper format. What I have on paper doesn’t also match what they sent electronically. So I can see the amendments made. There is a lot that are redacted.” [Family member]
“They’ve (the trust) magically handed my solicitors magical notes that reappeared out of nowhere after three years. Which we know are inaccurate because my mum was taking notes, I was taking notes at the same time. So we know the incorrect timings down to the point of where she, like time, she was born. So I’ve seen what they want to give me, but it’s so hard to even get your notes from them. Even if you’ve had an easy pregnancy and your child is still alive, you are battling to get these notes. It shouldn’t be like that. It shouldn’t have this kind of cloak and dagger over your notes. It’s personal information and you shouldn’t be held at gunpoint for wanting it.” [Family member]
- This approach from trusts is troubling from two aspects: first, it compounds the harm already suffered through trauma or bereavement; and second, it impedes the learning that should take place to prevent recurrence of similar incidents. It is essential that families are treated with compassion and honesty, and that learning and improvement are able to happen.
- Families also raised concerns that investigations did not always lead to improvements to care.
“The trust’s own internal investigation only identified very minor issues with my care, and after repeatedly providing much evidence to the Maternity and Newborn Safety Investigations programme (MNSI) into [name]’s death, they did eventually recommend nine safety changes to [the hospital] this summer, and all of these were in areas that we had alerted the hospital to long before. So now, nearly a year after [name]’s death, unfortunately, [the hospital] still haven’t enacted most of these safety recommendations, meaning that women and babies we live side by side with are still at risk today.” [Family member]
- Families often felt that they had no option but to pursue litigation when they were denied openness and honesty in the aftermath of harm and bereavement. They told us about the time they spent becoming experts in medical terminology and the law to enable them to make their case. The high costs of maternity litigation claims reflect the enormity of lifelong trauma for families and surviving children damaged by negligent care at birth. The current litigation process is long, expensive and inefficient, and could be contributing to defensive practice among some clinicians.
- Families told us that when things go wrong, they want to know what happened and why, explained in a way that they can understand. Families also expressed the importance of NHS trusts being accountable and of knowing that service changes will be made to prevent recurrence of preventable harm.
- We have heard from some families how much they valued independent investigations when things had gone wrong. We also heard from many families a desire for investigations to be undertaken independently from trust staff. Trusts sometimes try to achieve this by organising an independent review, but this is in the minority of instances.
- We have also undertaken some detailed interviews with families about their experience of coronial investigations, specifically whether coroners should have a role in investigating when babies are stillborn, and how this might help prevent future deaths. The terms of reference for the consultation led by the Ministry of Justice in 2019 focused only on babies who are stillborn at 37 weeks[41] gestation or later. But, after concerns raised by bereaved families, we agreed it was important to look more widely at when babies are stillborn, as many of the questions raised about coronial involvement apply once 24 weeks gestation is reached. In England and Wales, the law currently allows a coroner to investigate only when a baby is believed to have been born alive and then died.[42]
- Many families we spoke to whose babies were stillborn, had not received a full explanation of what happened from NHS investigations, despite there being processes in place, such as the Perinatal Mortality Review Tool (PMRT) and the Maternity and Newborn Safety Investigations programme (MNSI). They told us that the current system feels deeply unfair, can exacerbate trauma, and that the absence of a coronial investigation left them without answers about what had happened, returning home without their babies. They did not know if the deaths could have been avoided.
- We heard evidence from a number of families where there was ambiguity regarding whether their baby had been born alive. This ambiguity created distress and long-lasting trauma for families as they struggled to deal with the fact they were given no clear explanation for the death of their baby, precisely because their baby was deemed to be stillborn. To compound this, some parents were tormented by the thought that they had seen signs of life, but staff had not recognised this. Some families said that declaring their baby as stillborn diminished their baby’s life. They felt the system incentivised the recording of deaths as stillbirths as this prevents the case from being investigated by a coroner.
“I’ve still never agreed he was stillborn. He was resuscitated for 30 minutes before we were told he had died. You don’t resuscitate a stillborn baby. But you register a baby as stillborn, you have no investigation, an independent investigation. […] The bereavement midwife came with [name]’s stillbirth paperwork and gave them to me. I said, “[name] was not stillborn, he was neonatal”. And she said, “Well, this is what he’ll be registered as, and if you don’t register him as stillbirth, you won’t be able to have a funeral and you won’t be registered anywhere” […] You’re constantly fighting because of the stillbirth registration, because they’ve been able to hide behind it. That’s what I truly believe that they’ve hid behind that. He’s not in the public domain, his death isn’t in the public domain.” [Family member]
- Some families who have been through the coronial process following a neonatal death reported finding the process adversarial and difficult, with one family describing it as “brutal”. However, others have reported it as “cathartic”. We heard about distrust of how NHS trusts engaged with the coronial process and the imbalance of legal resources available to trusts compared with families.
The quality of estates
- Buildings are an important element of delivering modern maternity and neonatal care. The quality of the estate in which services are delivered directly affects the ability to provide safe and effective care, protect dignity and manage infection control.
- From our visits to the 12 NHS trusts, we have seen maternity and neonatal services that are delivered in estates that are outdated and dilapidated, and estates which are new and modern. However, a modern estate does not always equate to a high-quality service, for example, we have also seen examples of recently built estates which were misaligned with clinical and patient need. In some of the 12 trusts we visited, operating theatres were located on different floors from the maternity services and some rooms left women isolated from staff areas. We also heard from staff about the impact estates can have on the standard and quality of care that can be delivered, and on their morale.
- We were told of rooms being consistently out of action due to leaking roofs, restrictions placed on buildings due to fire hazard risk (meaning that clinical care can be compromised due to limits on the numbers of patients being able to be moved to the ward), delivery units that were cold, and corridors where there wasn’t enough space to navigate a hospital bed. Staff have told us how basic repairs are often delayed and how the volume of paperwork required to repair or replace a basic piece of equipment is burdensome, taking away the time that could be spent giving care.
“They include the weather report in their handover on labour ward because they have to be ready for heavy rain because of the numerous leaks.” [Staff member]
- During our site visits we have seen examples of rooms simply not large enough to accommodate staff and equipment – including Resuscitaires which are required for providing extra support to newborns. In one visit, we were informed that when an instrumental vaginal delivery was required in the delivery room, the door had to be left open to provide enough space – with a screen placed outside of the room to protect families’ privacy. It is inconceivable that anyone would choose to give birth in such a manner. We have to ask ourselves how this can be regarded as acceptable in 2026?
- We also saw maternity facilities where there were no or a limited number of ensuite toilets, and showers located some distance from the delivery room. For example, we heard of women having to use a bedpan during labour or having to walk down a shared corridor to have a shower in their bloodied hospital gowns immediately after birth. This lack of dignity can have lasting impacts on women and families.
- Some families also told us about the impact of a lack of facilities for non-birthing partners:
“…I was then transferred to the ward and my husband had to go home because it was 3am and he wasn’t allowed to stay. I was on my own with this child… she wasn’t feeding… I didn’t know what I was doing. Someone needed to be there.” [Family member]
“Even when you have visitors, you’re still in your little bed, your little box. There’s no seat for a visitor. So where are they sitting — on your bed?” [Family member]
- In some neonatal units we saw cramped facilities that did not allow for parents and families to be included in the care of their newborn in line with the Family Integrated Care (FiCare) model. Families have shared examples where a lack of space in neonatal units inhibited their “ability to have your child out for a cuddle safely because of just the space limitations” [Family member]. In one unit we saw that a chair provided for family use had to be moved around the room for different families and that staff and families were bumping into each other as staff tried to deliver care. Some of the family facilities we saw were dark, cold and unhospitable. This also contributes to poor infection control.
- Families have told us how estates can improve their experiences and enable Family Integrated Care, through facilities such as kitchen spaces, shower and sleeping facilities for partners and spaces for siblings to visit enabling a more positive family experience. This can especially impact families who have babies on the neonatal ward and may have to spend weeks, if not months, visiting the ward.
- We have witnessed how spaces and support for bereavement care are inconsistent. We have seen some bereavement spaces that offer quiet spaces that give families private areas and gardens to grieve and spend time with their baby. However, we have also seen trusts that do not have sufficient bereavement spaces and one hospital that did not have any at all. Some families have shared how the bereavement facilities and support they have received has had a positive impact on their experience. Other families have told us about experiences which heightened their trauma and loss, for example, cold cot facilities not working, of listening to nearby babies crying whilst they are mourning their own baby, of having to receive care in a ward shared with women in active labour, or being transported through delivery units.
“And I — when we moved from that room to another room, I said — because [name] was on me at this point, and I remember saying, “I don’t want to scare anyone else”, because I knew that they were going to wheel me through delivery suite, and I remember saying to them, “I don’t want other mums seeing us, like, I don’t want to scare them”. And a midwife said, “Nobody will know, nobody will look at you and know. You just hold her, and nobody would know”. […] I had to go through delivery suite, and I could hear mums in labour, I could — it’s all I could hear.” [Family member]
Workforce
- At its most fundamental, maternity and neonatal care must offer a safe service and staffing levels are key to ensuring that this is possible. Safe care requires an appropriate skill mix, supervision, relational continuity and psychological safety.
- Midwife staffing numbers are determined by Birthrate Plus, a tool to calculate staffing levels. Even in NHS trusts that have achieved full staffing according to Birthrate Plus, staff report that maternity units do not consistently feel safely staffed in practice, due to factors such as high turnover of staff and because the numbers include midwives who do not provide frontline care. In addition, the effects of inequality and deprivation affect staffing requirements. A recent review of Birthrate Plus has confirmed the robustness of the method but suggested further work needs to be done to consider these effects. We have also heard of the pressures resulting from midwives being moved away from critical areas to fill more specialised roles.
- Women and families have told us how the care they receive from staff leaves a long-lasting impression and can make the difference between leaving the hospital traumatised or reassured and supported. Some women and families recognised that staff are often working beyond capacity and that staffing levels impact on the quality of care provided.
- Staff told us of their desire to give quality care to patients. However, we also heard about unacceptable instances where staff have made cruel or insensitive comments to families when they are most vulnerable, including after a bereavement. In one instance, a doula supporting a mother described: “Her waters had gone, and she was just waiting for things to kind of start… she waited a few hours and then she went in, and I went in with her, and the consultant who met us kind of barked at her, actually, and said, ‘Well, why didn’t you come sooner? Are you stupid?’” “Now, how can you accept care from somebody who is so dismissive of you, and who talks down to you, and is so condescending?”
“In terms of bereavement, we said what his name was and everything, but she still got it wrong. She just wasn’t really listening. It’s like we were kind of again, just like we were rushed, like they just wanted to get rid of us and nobody really took that time to sort of give us that care really. […] we were getting to that point of leaving and the bereavement lady kept coming in and kept sort of like rushing us. She came in with a box of injections that I needed and interrupted our goodbyes. Then as we were leaving, we were told, make sure you cover his face because you don’t want to upset anybody.” [Family member]
- Despite recent staffing increases[43] and a decrease in the birth rate[44], we heard how the increasing complexity of maternity and neonatal services creates a highly pressurised work environment. We heard of poor morale, incivility and stress across clinical teams and examples of tensions between staff groups being witnessed by patients causing discomfort and anxiety.
- Unlike medical staff, midwives in specialist or managerial roles can have often have little or no involvement in direct clinical care depleting the number of midwives that can assist at times of high acuity and causing further frustration among front line staff. This is contributing to the loss of experienced frontline staff, destabilising teams and compromising the quality and consistency of care being provided. This is compounded by some staff reporting that they have received training which is reactive and questioning its effectiveness.
“A couple of years ago we had one where we had an external agency come in and it was mandatory training for all of our staff to do a two day training course. And everybody had to do that course which was an online course on culture and cultural >awareness and improving behaviours. It was okay, do I think it’s made any difference? No. I didn’t think it was going to make any difference at the time when it was done, and I don’t think it has now.” [Staff member]
- We have observed how the medical cover provided in maternity units is inconsistent across the country; this is made more complex by doctors providing maternity care frequently covering gynaecology services in addition, especially in smaller units. Resident and consultant medical staffing patterns differ substantially between trusts with some units reporting difficulty maintaining safe obstetric rotas, particularly overnight or at the weekend. The lack of senior input left families without information at critical moments when important decisions had to be made.
- Neonatal staff have also told us about the difficulty in filling neonatal nursing roles and this adding increasing pressure for teams on shift. We have also heard about the impacts of reduced midwifery cover at night and on weekends on women and families where their experience is that specialist care, such as bereavement or breast-feeding support, is not available due to it being ‘out of hours.’
- One family described not having access to bereavement support for days after their baby died, ‘so we lost on the Friday and it wasn’t until Monday that we had any specific bereavement care because the bereavement midwives just work office hours. [….] baby loss doesn’t happen in office hours only’. [Family member]
- Conversely, good quality bereavement support delivered in an appropriate environment can have a positive impact on the ability of families to come to terms with their loss. One family described the outstanding support they received from bereavement midwives following the discovery that their baby had died in utero. The “professional love” they experienced made it “hard to leave the hospital” but ultimately made a significant contribution to coming to terms with their baby’s death.
Part 3: Next Steps
- As I said in my foreword, the system is not working for women, babies and families or for staff. We have seen and heard about problems at every stage of the maternity and neonatal journey. Safe and equitable maternity and neonatal care does not begin at the hospital door, nor does it end at discharge. Families have frequently described their care as episodic rather than continuous. For women and families experiencing trauma and social disadvantage, this can undermine trust, delay escalation of concerns and increase psychological harm.
- Some families have been critical that the investigation has wanted to hear about the full range of experiences that women, birthing people, families and non-birthing partners have of maternity and neonatal care. I recognise the concern that negative, traumatic and distressing experiences will not be heard or will be diluted by taking this approach and I want to reassure bereaved and harmed families that they remain front and centre of this investigation.
- Some staff have expressed concern that the daily pressures and negative experiences they face are not being sufficiently recognised. In identifying those broader challenges, I am not excusing poor behaviours, but it is important to understand the landscape in which staff are operating.
- By taking a family first, whole system approach which understands different perspectives, my intention is to craft recommendations which will enable a step change in the provision of maternity and neonatal services in England, rooted in the delivery of safe, consistent care.
- There are a number of additional areas of work which will be taken forward in the next phase of the investigation. This includes concluding our analysis of previous recommendations made to improve maternity and neonatal care. We will also take evidence from national stakeholder organisations, which will provide us with insights into governance and organisational structures, training, regulation and funding pathways for the different elements of maternity and neonatal services. We will also hold further evidence panels focused on inequalities, system wide working and the relationship between trusts and families.
- Families are invited to continue to contribute to the investigation via our calls for evidence. The public call for evidence for women and families is open until 17 March 2026 (Call for Evidence – National Maternity and Neonatal Investigation). There are two different surveys available: one for women and people who have been pregnant to share their own experiences of maternity and neonatal services, and one for other people to share their experiences supporting someone through pregnancy. This could include fathers, non-birthing partners, family members, friends, or other support people.
- The call for evidence for staff working in maternity and neonatal services is open until 9 March 2026. Trust-specific links have been shared with senior executives in every NHS trust which provides maternity and neonatal services. All staff should be able to obtain this link from within their organisation.
- I realise that some of the experiences identified in this report may be concerning for women and families currently using maternity and neonatal services. If you have concerns regarding your own care, I would like to reassure you that whilst there are many instances of unacceptable levels of care, there is also good practice across the NHS. If you have concerns regarding your own care, I would encourage you to raise any concerns directly with your midwife or obstetrician, or with the leadership of your local trust.
- My team and I will now be focussed on completing our investigation and analysing all the evidence which has been, and will continue to be, made available to us in order to produce one set of national recommendations to drive improvements in maternity and neonatal services in England. The Secretary of State for Health and Social Care will then chair a National Maternity and Neonatal Taskforce whose role it will be to design and deliver an Action Plan informed by the findings of this investigation and its recommendations.
- It has been a privilege to meet with so many women and families and to hear their determination to drive change. I have heard from staff who want to make improvements and I have seen some evidence of change already happening. This gives me hope that these systemic problems can and will be overcome.
Annex A: Engagement to date
This section provides an updated overview of the work we have undertaken since the publication of the investigation’s Terms of Reference in September. My team and I have:
- Met 295 families including through 40 family panels and 3 blended lived experience and community panels as part of the local investigations. 10 further family panels are scheduled to take place in late February and March. These are additional panels to ensure we hear from a diverse range of women and families in each locality.
- Held individual interviews with over 65 bereaved and harmed families. Family interviews will continue to take place until the evidence submission deadline in mid-March.
- Launched a call for evidence for the public. This has two surveys, one for women and people who have been pregnant, and one for people who have supported someone through pregnancy. The surveys have received over 8,000 responses from women and families, and we continue to work with organisations to publicise the call for evidence as we aim to reach as many women and families as possible before the closing date of 17th March.
- Held 7 evidence panels with families and with voluntary and community organisations as part of the system-wide and inequalities work. A number of further panels are scheduled to take place in late February and March with communities which have been identified as facing health inequalities or inequalities in experiences and outcomes in maternity and neonatal care specifically. This will include hearing from Black, Asian and other marginalised communities for example LGBTQ+ families, and hearing about specific aspects of care, for example neonatal care and experience of mental health services.
- Met with 15 MPs and the Maternity All-Party Parliamentary Group (APPG) as part of the system-wide review and inequalities work. Meetings with MPs have been to directly take evidence and/or to identify ways MPs can support the investigation to engage with women and families. Evidence sessions with the Black Maternal Health, Baby Loss, Birth Trauma, and Patient Safety APPGs are due to take place in March.
- Held 44 staff panels and completed 75 staff / executive interviews as part of the local reviews.
- Opened a call for evidence for staff working in maternity and neonatal services in NHS trusts. This is being distributed via NHS trusts and has received over 6,700 responses to date.
- Conducted 12 interviews with national stakeholders as part of the review of the legal framework regarding the role of Coroners in relation to stillbirths and compensation following harm caused by clinical negligence. Further stakeholder interviews are planned for March.
References
[1] We have talked to: women, non-birthing partners, families, friends, staff, NHS trust leaders, community and advocacy organisations, MPs and All-Party Parliamentary Groups. In the next phase of evidence gathering we will take evidence from national organisations including the Royal Colleges and regulatory bodies.
[3]NHS England & NHS Improvement (2018). The Perinatal Mental Health Care Pathways.
perinatal-mental-health-care-pathway.pdf
[4]MBRRACE- UK, Maternal mortality 2022-2024
[5] The NHS Constitution for England – GOV.UK
[6] Child and infant mortality in England and Wales – Office for National Statistics
[7] MBBRACE- UK, Maternal mortality 2022-2024
[8] Sources: Office for National Statistics – Births in England and Wales (2024), Child and infant mortality (2008-2023), Mortality Statistics: Childhood, infant and perinatal (1999-2007)
Note: Due in part to a 2019 update to British Association for Perinatal Medicine guidelines on providing survival-focused care to extremely premature babies[8], the number of babies born before 24 weeks of pregnancy (the point at which RCOG considers a baby to be viable, or able to survive outside the womb) who showed signs of life has increased from 0.11% of live births in 2010 to 0.15% of live births in 2024. Around 4 in 5 of these babies sadly die in their first month of life, and because of this the neonatal mortality rate for babies born at any gestation shows a different trend than the neonatal mortality rate for babies born after at least 24 weeks of pregnancy.
[9] Office for National Statistics (ONS), Births in England and Wales: 2024
[10] NHS England, NHS Maternity Statistics
[11] Maternal mortality 2022-2024 | MBRRACE-UK | NPEU
[12] MBBRACE- UK, Maternal mortality 2022-2024
[13] NHS England, NHS Maternity Statistics
[14] NHS England, NHS Maternity Statistics
[15] Caesarean sections | OECD
[16] Births in the United States, 2024 – NCHS Data Briefs – NCBI Bookshelf
[17] Maternity and neonatal services in East Kent: ‘Reading the signals’ report – GOV.UK
[18] FINAL PRESS RELEASE INDEPENDENT MATERNITY REVIEW OF MATERNITY SERVICES REPORT PUBLISHED 3032022.docx
[19] NHS England, NHS Maternity Statistics
[20] Mannion R, Davies H. Understanding organisational culture for healthcare quality improvement BMJ 2018; 363 doi: https://doi.org/10.1136/bmj.k4907 (Published 28 November 2018)
[21]Professor Michael West, King’s Fund,2017) in NHSE Why is culture important (2017)
[22] Mannion R, Davies H. Ibid
[23]Inquiry into racial injustice in maternity care – Birthrights
[27] MBRRACE-UK, Perinatal Mortality Surveillance: UK perinatal deaths of babies born in 2023
[28] Office for National Statistics (ONS), Births in England and Wales: 2024
[29] National Maternity and Perinatal Audit, Ref 308 Inequalities Sprint Audit Report 2021_FINAL.pdf
[30] MBRRACE-UK, Perinatal Mortality Surveillance: UK perinatal deaths of babies born in 2023
[32] Maternal mortality 2022-2024 | MBRRACE-UK | NPEU
[33]Published work further reflects how the awareness of disadvantage adds pressure to ethnic minority families to be well informed and ready to ready to advocate for themselves in attempt to achieve safe and respectful care: Confidence in maternity care services: engagement with ethnic minority women and maternity staff – GOV.UK
[34] Black Maternity Experiences Report 2025 — FIVEXMORE
[35] (Birthrights have described this stigmatisation as Black and Brown bodies being regarded by professionals as ‘defective’ and a risk to be managed.)
[36] The Muslim Women’s Network reports that 1 in 5 Muslim women report their maternity care as ‘poor’ or ‘very poor’ with many feeling that they were treated differently due to their race, ethnicity, Muslim faith and age Muslim Women Network
[37]Birthrights Dignity in Childbirth survey found that 56% of disabled women felt that health care providers did not have appropriate attitudes to disability and only 19% of women felt that reasonable adjustments had been made for them: Disability – Birthrights
[38] Experiences of women from ethnic minorities… | NIHR Open Research
[39] Published reports highlight how lack of interpretation results in women being unable to understand, make informed decisions and consent to their medical care: Confidence in maternity care services: engagement with ethnic minority women and maternity staff – GOV.UK
[40] Maternity care experiences of women with physical disabilities: A systematic review – ScienceDirect
[41] https://consult.justice.gov.uk/digital-communications/coronial-investigations-of-stillbirths/
[42] The Coroners and Justice Act 2009, s.1(1)
[43] NHS workforce statistics – NHS England Digital
[44] Births in England and Wales – Office for National Statistics